


Is your dental implant giving you sinusitis?
The sinuses, or more correctly the paranasal sinuses, are air-filled bony chambers within the facial bones of the skull. There are four paired paranasal sinuses in the human skull and they have an inner lining or mucous membrane that is continuously producing mucus.
The paranasal sinuses https://www.webmd.com/allergies/picture-of-the-sinuses#1
It is estimated that the average human being produces approximately 150 millitres of clear mucus a day. When these sinuses get infected, mucus production increases and the colour often turns yellow or green. Infections of the sinuses is called sinusitis. There is often pain and pressure felt over the cheek and forehead. Patients feel congested or stuffy, they lose their sense of smell and can run a fever.
Unfortunately, the term “sinus” means something very different to the lay person. Many patients who consult me, often complain that they have a long history of “sinus” or “morning sinus”. What they mean is a runny or blocked nose in the mornings with sneezing. This is often due to an allergy and should be correctly referred to as allergic rhinitis. The nose may be blocked and filled with mucus, but rarely are the sinuses affected! Scans of the nose often show swelling within the nose affecting the nasal turbinates but no evdence of sinus obstruction of thickening of the sinus lining.
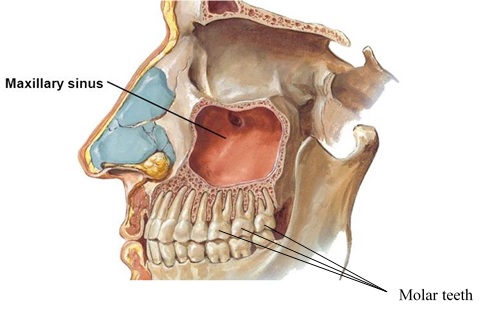
Root of the molars lie close to the floor of the cheek (maxillary) sinus https://www.drmassoomi.com/blog/sinus-lifts-and-dental-implants/
Sinusitis is due to a sinus infection. Most infections result when the flow of mucus out of these bony air-fiiled chambers is obstructed. Mucus stagnates and an infection ensues. Bacteria normally enter the sinuses through the nasal passages. However, a small proportion of cases of sinusitis (about 10%) are due to infections entering the cheek sinus (maxillary sinus) through the teeth. This is because the roots of the teeth project into the floor of the maxillary sinus. The floor of the cheek sinus has a dense membrane called the Schneiderian membrane that forms a barrier against dental infections, but in some cases this barrier breaks down.
Amongst people in their 40s and 50s, newly onset sinusitis often has a dental cause. In fact, amongst people presenting with one sided cheek sinus infections (maxillary sinusitis), about 75% will have a dental origin. In a third of these cases, dental root or gum infections (periapical or periodontal infections) is the source. However in the majority – almost two-thirds – dental surgery is to blame. Procedures such as dental extractions, dental implant placements and sinus augmentation grafts (or a “sinus lift” procedures) can inadvertently damage the Schneiderian membrane and leave a root for bacteria that normally inhabit the mouth to enter the cheek sinus. The first molar is most often the tooth involved, followed by the second and third molar and the second pre-molar.
In two-thirds of cases, patients do not report any dental pain. The the time lag between dental surgery and the presentation of symptoms of sinusitis can be up to 4 years!
Pus from the left nasal cavity in a patient with left cheek sinusitis (odontogenic maxillary sinusitis
Sinusitis due to dental infections or dental surgery is called odontogenic sinusitis. Other than the one-sided nature of symptoms, the species of bacteria isolated from the sinuses often originate from the mouth. The pus is often very foul smelling and thick. Repeated courses of antibiotics often don’t work. In many cases, as dental surgery can pre-date the onset of sinuistis by several years, the family practitioner or the ENT surgeon may not think to look for a dental cause. In fact in my experience, about half of patients who clearly have dental source to their sinusitis cannot even recall having dental surgery!
Simple dental xrays can miss up to 60% of dental root problems that lead to sinusitis. Cone-beam CT has a better sensitivty and should be part of a thorough dental assessment by an experienced oral surgeon.
Once a diagnosis is made, it is important to treat the underlying dental problem first and mamage the sinusitis medically with nasal irrigation, antibiotics and nasal steroid sprays. In early cases, sinus surgery mat not be necessary. One study estimated that 52% of cases of maxillary sinusitis can be managed this way. If however there is presence of a dental foreign body in the sinus or involvement of the sinus drainage pathway (known as the ostiomeatal unit), the endoscopic sinus surgery may be necessary
Case study
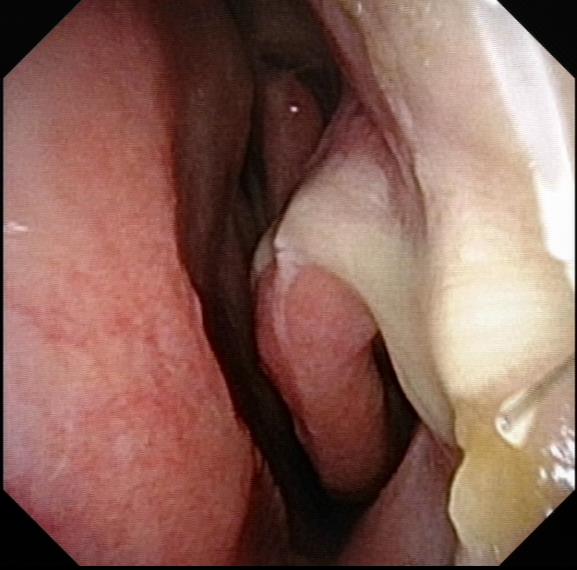
Examination with a nasal endoscope revealed a small streak of thick pus from the left cheek (maxillary) sinus
A 29 year old woman presented with a 7 year history of ‘sinus’. She described left nasal congestion with sneezing, and a persistent thick yellow nasal discharge with a post-nasal drip. More recently, she has developed left sided toothaches. She had seen two dentists and was given the ‘all clear’. Dental xrays were ‘normal’ but had revealed sinusitis. My own examination revealed left sided sinusitis. There was pus in the left nasal cavity coming from the entrance to the left cheek (maxillary) sinus. A subsequent CT scan showed sinusitis affecting the left maxillar sinus alone.
She was referred to a dental surgeon who treatment her first molar. Despite this, her sinusitis did not resolve and she required endoscopic sinus surgery under general anaesthesia. This was a simple procdure that took no more than an hour.
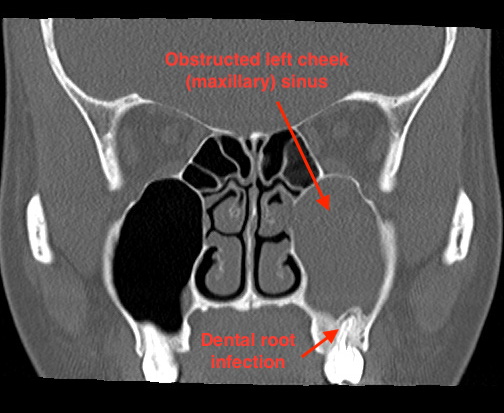
A CT scan of the sinuses showing an obstructed left cheek (maxillary) sinus) and the dental source of the sinusitis
At her final review a few months after surgery, the patient had made a complete recovery. I had fashioned a large opening into her cheek sinuses and the pictures below show that they remain healthy and patent.
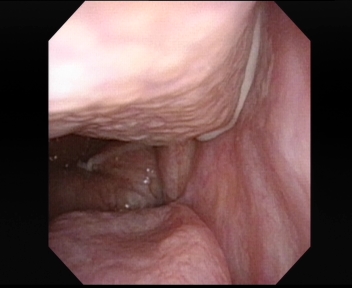
The left middle turbinate which guards the entrance into the left sided sinuses. The openings visible are into the ethmoid sinus

Lining of the cheek (maxillary) sinus

The ledge between the cheek sinus and the nose
Reference
Odontogenic Sinusitis: A Review of the Current Literature. Little RE et.al. (Laryngoscope Investigative Otolaryngology 3: April 2018) see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5915825/pdf/LIO2-3-110.pdf
Share this blog via:


