


What to expect after my child’s tonsillectomy
Tonsil removal or tonsillectomy is a common operation undertaken in young children. The tonsils lie on the sidewalls of the throat between two “pillars”. These pillars are actually muscles (the palatoglossus and palatopharyngeus to be precise!). Tonsil removal can be undertaken in many ways. One method involves the use of controlled ablation (or coblation) which offers reduced pain and therefore a quicker return to normal diet and activities. The operation is done through the mouth. The child is laid on their back and following induction of general anaesthesia and intubation (placement of a breathing tube into the windpipe), a mouth gag is placed.

Large tonsils in a child. These tonsils were causing airway obstruction

The typical mouth gag positioning for a tonsillectomy. The surgeon sits at the head of the child
Surgery takes about 30 minutes. I often inject a local anaesthetic solution which comprises both an anaesthetic (2% Lidocaine) and adrenaline which reduces bleeding. I use coblation technology which generates temperatures around 70 degrees Celsius and therefore causes less pain post-operatively. In selected cases, electrocautery is necessary to seal blood vessels. I usually finish the operation by placing swabs soaked in a long-acting anaesthetic (Bupivacaine) into the tonsil bed. They are left there for a full minute. Each surgeon has their own preferred method of surgery and I have developed a repertoire that seems to produce the least amount of discomfort without compromising safety and efficacy.
Operating theatre
Parents of young children will be allowed to come into the operating theatre with their child and remain there until the child is fully asleep. We use inhalational anaesthesia for children so there are no needles or injections necessary until the child is fully asleep. A mask is gently placed over the child’s nose and mouth and the gas used is often flavoured with vanilla or strawberry essence! Parents are encouraged to help place the mask themselves on children that are fretful.
Once the child is asleep, parents are escorted to a waiting area during the surgery. As most would have been fasting with their children, there is time for a quick bite at this point! When surgery is done, you will be called and ushered into the recovery area. Your child may be asleep or partially awake. They will often cry upon waking – it is more likely to be due to the disorienting effect of surgery rather than excruciating pain. If your child is asleep, they will be placed in the recovery position i.e. on their side. Once the nurses in the recovery area are happy, your child will be transferred with you to the wards.
Ward
Once you and your child are back on the wards, the nurses will monitor your child. They will be checking for any bleeding, nausea, vomiting and pain. The anaesthetist would have given your child painkillers in the operating theatre. This includes a small dose of steroids to reduce post-operative nausea and vomiting, and a suppository (often paracetamol or diclofenac). If pain is still present, the nurses can give your child additional doses of painrelief.
We usually start children on sips of water or juice and then reward them with some ice cream! If all remains well after 1-2 hours, a soft diet is allowed – be it some porridge or soft bread. Chewing and swallowing after a tonsillectomy will feel odd to a child but if they are distracted by a tablet or TV they seem to soldier through!
Some children will be discharged on the day of surgery, but some will stay a night with us in the hospital. Very rarely, some children will need antibiotics or fluids in a drip.
Pain
Pain following tonsillectomy escalates in the first few days after surgery before waning. It is always worse at night and in the early hours of the morning. This is probably due to mouth breathing at night and reduced swallowing that dries the throat. Children may also sense pain in the ear. This is called referred otalgia and is simply due to the tonsil bed sharing a sensory nerve supply with the eardrum.
Here are some helpful pointers on how to manage the pain
- Painkillers. Your child would have been discharged with paracetamol and ibuprofen. I usually advise taking paracetamol before meals so that eating is relatively free of pain. If there is pain after a meal, do give them a dose of ibuprofen. For children who are used to suppositories, do consider a suppository overnight to help with pain relief. Older children may also manage throat sprays or gargles. In general, the younger ones cannot gargle and hate sprays in the mouth!
- Diet. Eating and chewing help the pain get better. Try to progress to solid food as quickly as possible after discharge. I usually suggest parents offer their children whatever they want – even if it may be fast food! The act of chewing relieves the spasm in the throat and jaw muscles and eases the pain. A “matronly approach” is advocated i.e. the child doesn’t leave the dinner table until their plate is empty! I know full well that this is difficult but one has to be cruel to be kind! Missing a meal is a recipe for disaster as it makes the next meal even harder for the child
- Fluids. Encourage your child to drink lots. Ideally constant sipping of water or juice through the day. Too much dairy often thickens the phlegm so I would advise moderation with milkshakes and yoghurt. Sparkling water is a particularly good thing as the fizzy nature helps clear the tonsil beds
- Antibiotics. You would have been discharged with antibiotics and it is important to complete the course. Probiotics may help reduce complications of antibiotics. There is evidence that antibiotics reduce pain scores
- Ice collar. This is something advocated by some childrens’ hospitals. A simple “fever pack” placed on the throat is helpful to some children
Physical Activity and School
I usually advise that your children avoid strenuous activities for a week following tonsil surgery. Going out into the playground is fine after 1-2 days. Swimming is fine too for children who have only had their tonsils removed. I usually suggest children who have had grommets inserted, or adenoids removed, not swim for 1-2 weeks. Returning to school is fine after 7-10 days. It really varies between children. Some children are better off back at school sooner rather than later!
The ‘Dip’
It is well described that some children have worsening pain or just seem a little off between days 5-7 following surgery. They often sleep poorly. This is probably an effect of a low-grade infection. One may need to take things a little slower during this period and return to a softer diet with more fluids and painkillers for a while.
Throat appearance
Some parents will look into their child’s throat following a tonsillectomy. You will see an accumulation of yellow material in the tonsil beds. This is called slough. This is normal and is not an infection. Slough is, however, a nutrient for bacteria, and eating solid foods helps your child shed this slough faster.
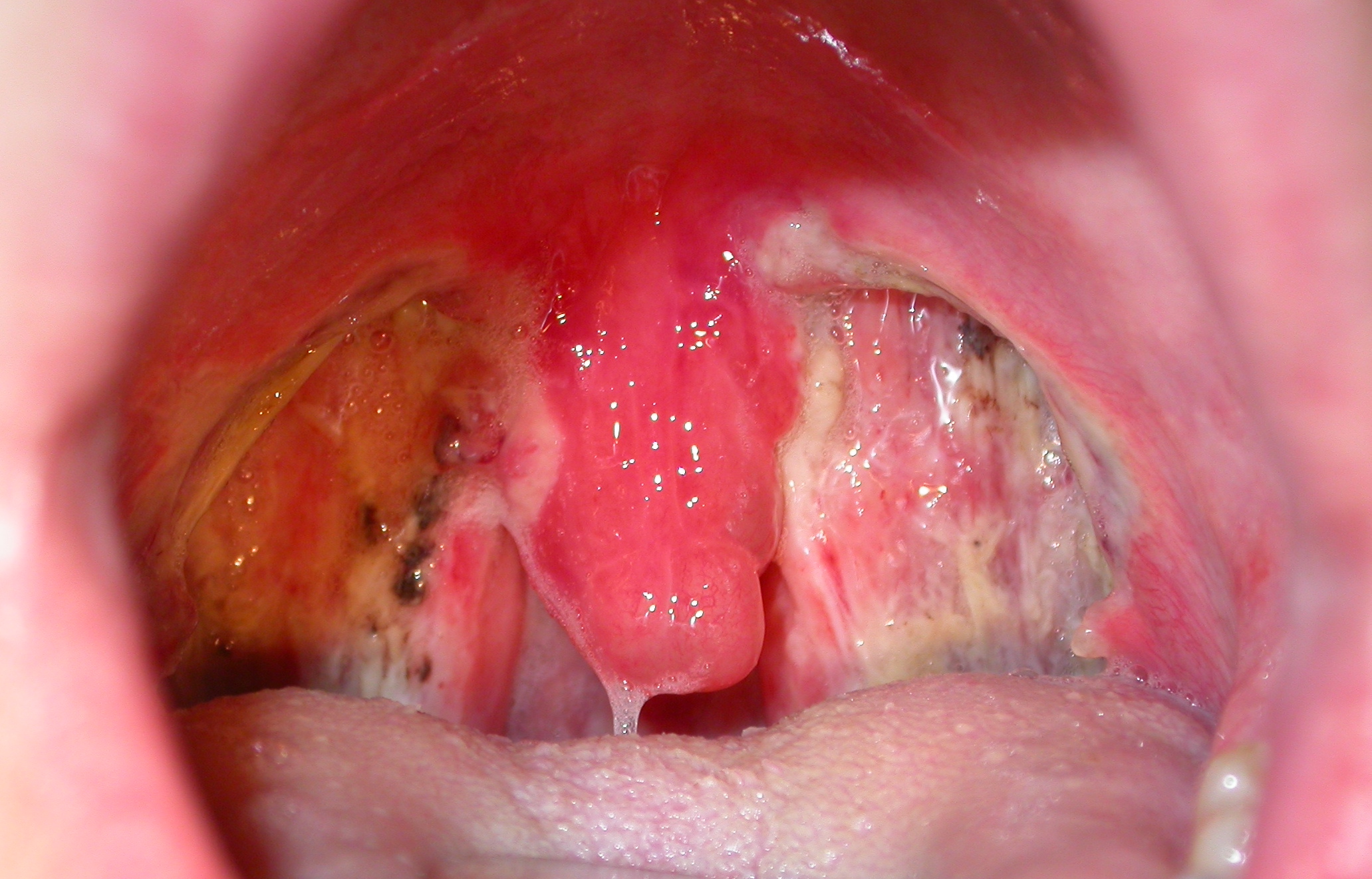
The tonsil bed coated by slough
What to look out for
There are a few adverse events that may happen following a tonsillectomy. It is important to bear these in mind
- Bleeding. Post-tonsillectomy bleeding is an unfortunate sequela to surgery in some children. Bleeding may vary from small amounts of blood-stained saliva that the child spits out or more significant bleeding. The incidence of bleeding in children following surgery is about 2.9% and it often occurs between days 6-10 following surgery. If bleeding does occur, do have a look at your child’s mouth and throat. If there is fresh blood or a large dark clot, it is best to contact the clinic or come to the hospital’s emergency department immediately. The staff there will make an assessment and contact me. A few children may need to be taken back to the operating theatre to stop any persistent bleeding. This rate is less than 1%
- Fever. A fever despite antibiotics is unusual. Do contact the clinic should this occur
- Diarrhoea. This is probably a side effect of antibiotics. If it is severe you may have to stop the antibiotic course. Please contact the clinic to inform us
- Uncontrolled pain. In a few children, the painkillers may have little beneficial effect and food and fluid intake is severely reduced. Some children will need to be readmitted for intravenous fluid and pain relief. This is exceedingly rare
- Breathing difficulty. Some children find that they have mild difficulty breathing when lying on their back. This is due to swelling of the palate and uvula that often occurs after tonsillectomy. This will always resolve but you may want to place your child on their side when asleep
Most children are back to a normal diet and activities after 5-7 days. Few children will have any lingering symptoms beyond day 12.
I hope this information is helpful. Whilst a lot of information here is from learned medical journals and textbooks, the really useful stuff is what I learn from parents! So if you feel I have missed something out and wish this communicated to other parents, please do email me at drjeeve@entclinic.sg
END
Share this blog via:


