


Sudden Hearing Loss

Sudden hearing loss is a medical emergency to ENT Specialists. It is important to establish the cause of any hearing loss urgently. Hearing loss may be due to problems in the ear canal or middle ear such as ear wax or middle ear fluid (effusion). This is called conductive hearing loss as the conduction of sound to the inner ear is impaired. Rarely, hearing loss is due to damage to the inner ear. This is known as sensorineural hearing loss. Sudden sensorineural hearing loss is one of the few ENT emergencies that require prompt action. Early diagnosis and treatment can prevent the irreversible loss of hearing.
Sudden sensorineural hearing loss (SSNHL) is defined by ENT Specialists as a rapid deterioration hearing (specifically 30 decibels or more in three contiguous frequencies) over 3 days or less. Most patients have not had a hearing test prior to the onset of hearing loss, so we usually compare hearing levels in the affected ear with that of the normal unaffected ear.
How do I know if I have Sudden Sensorineural Hearing Loss?
Sudden sensorineural hearing loss occurs rapidly and usually affects only one ear. To the patient, there is often no obvious cause such as a common cold, swimming, or the use of a cotton bud. There may be associated fullness in the ear or ringing (tinnitus). Some patients may also be dizzy or suffer vertigo.
The sudden onset of tinnitus that persists often distracts the patient and the doctor from underlying hearing loss. We see many patients who complain only of one-sided (unilateral) tinnitus but in fact, have an underlying hearing loss that is only diagnosed on clinical examination and hearing tests.
What should I do if I think I have Sudden Sensorineural Hearing Loss?
See a doctor urgently if you have all the features of sudden sensorineural hearing loss. Most family doctors and emergency department physicians are aware of this condition and can institute treatment immediately. A thorough assessment should include an examination of the ear with an otoscope to exclude wax or infection as a cause of hearing loss. You should volunteer any relevant information such as any recent medication you have started (including cancer chemotherapy), high cholesterol, diabetes, and high blood pressure.
There are two simple tuning fork tests that any doctor should be able to perform. They are called the Rinne’s and Weber’s tests. If they suggest a sensorineural hearing loss then you will be started immediately on medication that will help reverse the hearing loss.
Many hearing aid centres will be able to undertake a hearing assessment (or audiometry) without the need for a specialist referral. It is important that audiologists or hearing aid dispensers exclude ear wax impaction or infection before performing any hearing tests. This ensures an accurate test result.
Referral to an ENT Specialist is always necessary if you have sudden sensorineural hearing loss. Several investigations are necessary and some treatments can only be undertaken by specialists.
What causes Sudden Sensorineural Hearing Loss?
There are various theories as to why people develop sudden sensorineural hearing loss. Studies have postulated vascular (blood circulation), viral infection or reactivation, and autoimmunity (immune system attack of the inner ear) as possible causes. In some patients, drugs are to blame. This can occur with certain types of chemotherapy for cancer and antibiotics for infection. A small number of cases are due to a benign tumour of the inner ear called a vestibular schwannoma.
It is said that a third of patients will have an underlying cause of their hearing loss that is not apparent at presentation. This suggests patients should be followed up long-term even if they fully recover from hearing loss.
How common is Sudden Sensorineural Hearing Loss?
Sudden Sensorineural Hearing Loss occurs in 5-27 per 100,000 people per year. It is more common in people aged 50-60 years old. This figure suggests that we should see around 250-1000 cases per year in Singapore. Many of these patients do not see a doctor. Fortunately, a good proportion will get better without any intervention so the resultant number of patients with permanent loss is small.
How is Sudden Sensorineural Hearing Loss managed?
Diagnosis
The diagnosis of Sudden Sensorineural Hearing Loss relies upon a good history and clinical examination of the patient. I cannot stress the utility of the humble tuning forks tests that I mentioned earlier. For any healthcare professionals reading this blog, the following video from the American Academy of Otolaryngology is a useful reminder on how to perform a good clinical examination of the ear. It includes the correct way of performing Rinne’s and Weber’s tuning fork tests.
Clinical examination is then followed by pure-tone audiometry performed in a sound-proof booth if this is available. In The ENT Clinic, we are fortunate to have sound-proof booths and state-of-the-art audiometric equipment to ensure your hearing thresholds are measured with great accuracy.
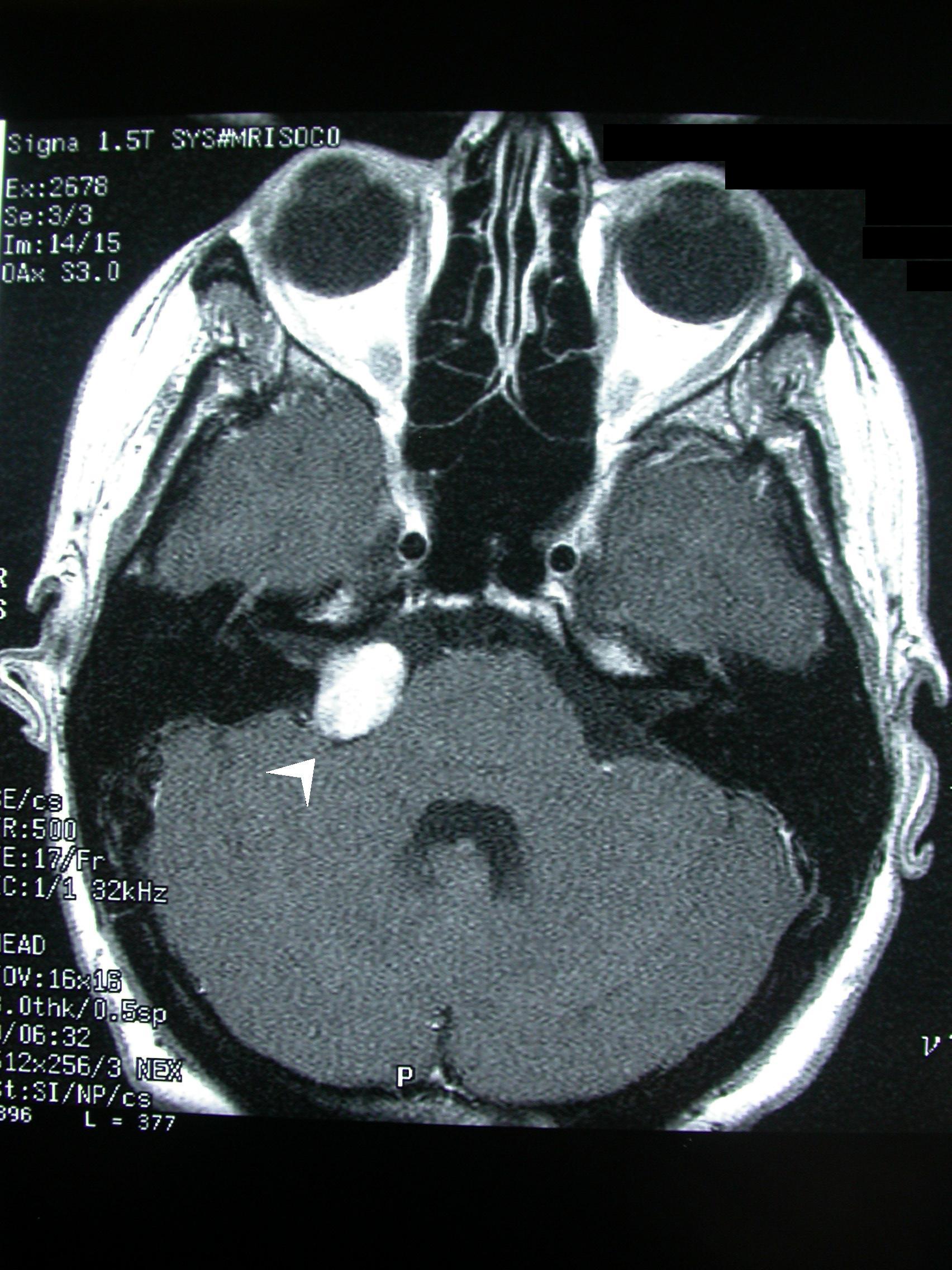
Patients with Sudden Sensorineural Hearing Loss should be offered an MRI scan to exclude a tumour of the inner ear called a vestibular schwannoma.
Blood tests should be considered selectively in patients who have sudden hearing loss to identify an underlying cause. Although evidence suggests that routine blood tests are not warranted, I tend to do these as they may pick up underlying diabetes, high cholesterol, or rarely an autoimmune cause.
Prognosis
The medical literature suggests that between 32-65% recover their hearing spontaneously (meaning without any treatment whatsoever). Patients who presented with more severe loss, who are older, and who have significant dizziness are likely to fare worse. In these patients, even if hearing loss recovers, persistent tinnitus poses a significant problem.
Most patients who recover their hearing tend to do so in the first 2 weeks. Those who recover half their hearing in the first two weeks do better and may enjoy continued improvement in hearing thresholds. Those who have no improvement in hearing in the first two weeks often do not show any significant improvement at all. However as case study 2 (vidē īnfrā) shows, this is not always the case!
Treatment
Oral Medicines
Once a diagnosis is confirmed, treatment should start immediately. The cornerstone of treatment is the use of oral steroids (Prednisolone or Dhasolone). Steroids should be started within 2 weeks of onset. There appears to be little benefit if commenced after 4-6 weeks. The usual dose is 1 mg/kg body weight per day (up to a maximum of 60 mg) of Prednisolone for 7-14 days and then tapered over a similar period of time. The dose should be taken as a single morning dose after food to keep gastric side effects and insomnia to a minimum. I often prescribe a proton pump inhibitor (e.g. Omeprazole, Rabeprazole) in conjunction.
Whilst evidence for other medications is lacking, many ENTs including myself add antivirals, vasodilators (medicines that increase blood supply to the inner ear), and blood thinners. These include Valacyclovir or Valtrex, Betahistine or Betaserc, Gingko Biloba or Tebonin Forte, and Aspirin.
Case study 1
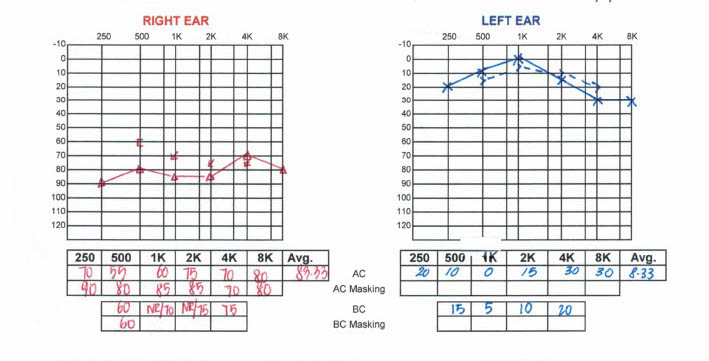
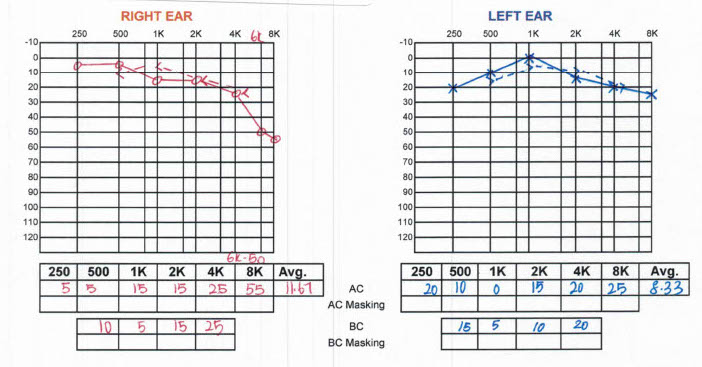
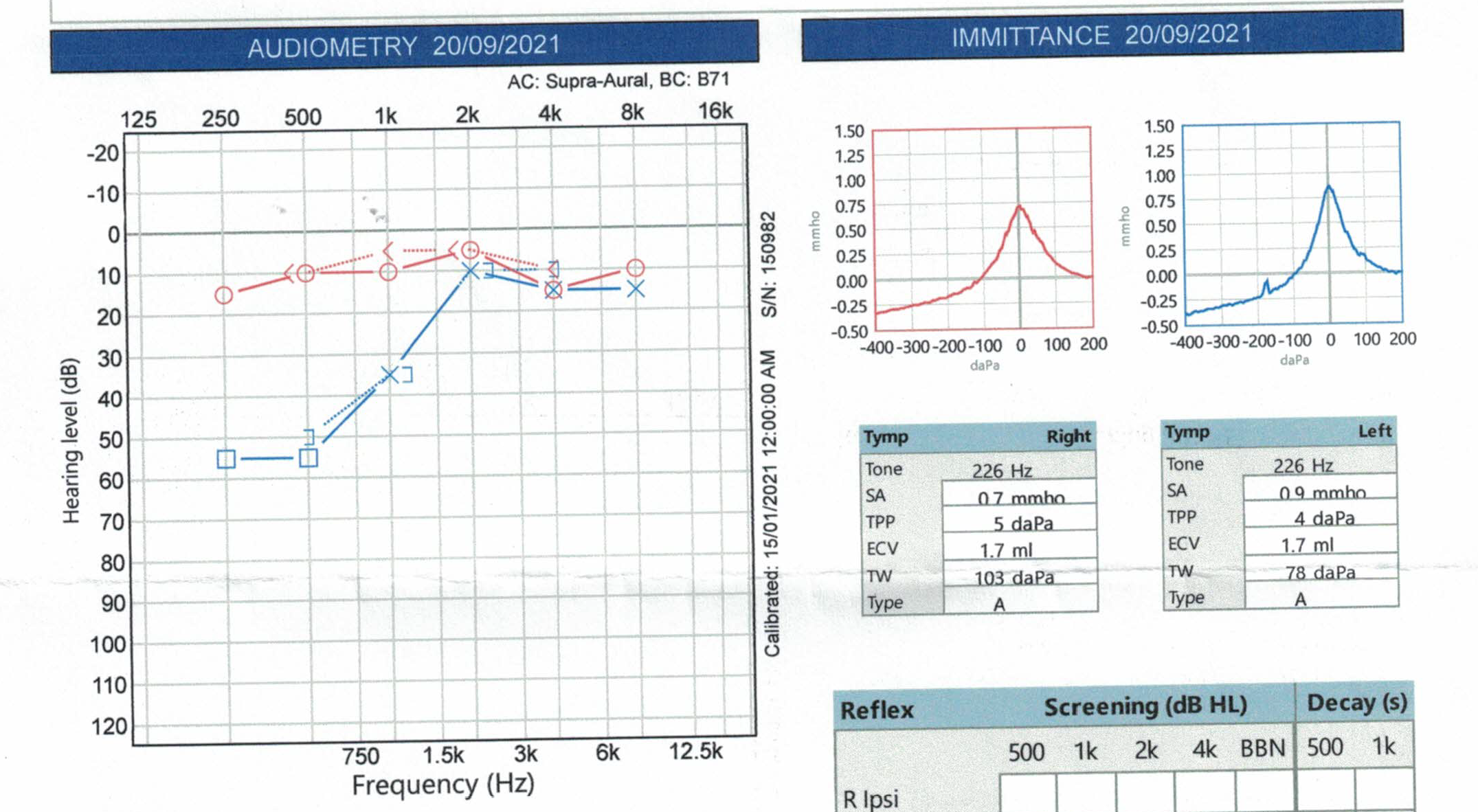
The audiogram below belongs to a 51-year-old gentleman who woke up at midnight on a Friday with sudden-onset ringing (tinnitus) in his right ear. He managed to fall asleep again but woke up the next morning with a sensation of blockage in the right ear. The tinnitus had resolved. He waited until Monday and saw a GP who gave him nasal sprays and decongestants. This first GP failed to assess his ear correctly and identify that the hearing loss was sensorineural in nature. Fortunately, he went to see another GP in the Tanjung Rhu area who is exceptional in his clinical acumen. This second GP correctly diagnosed his condition and promptly sent the patient to me.
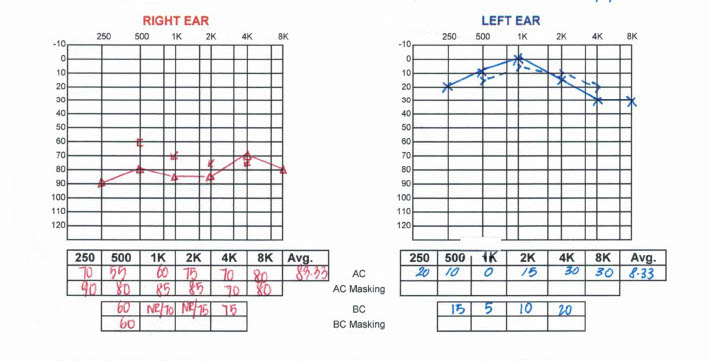
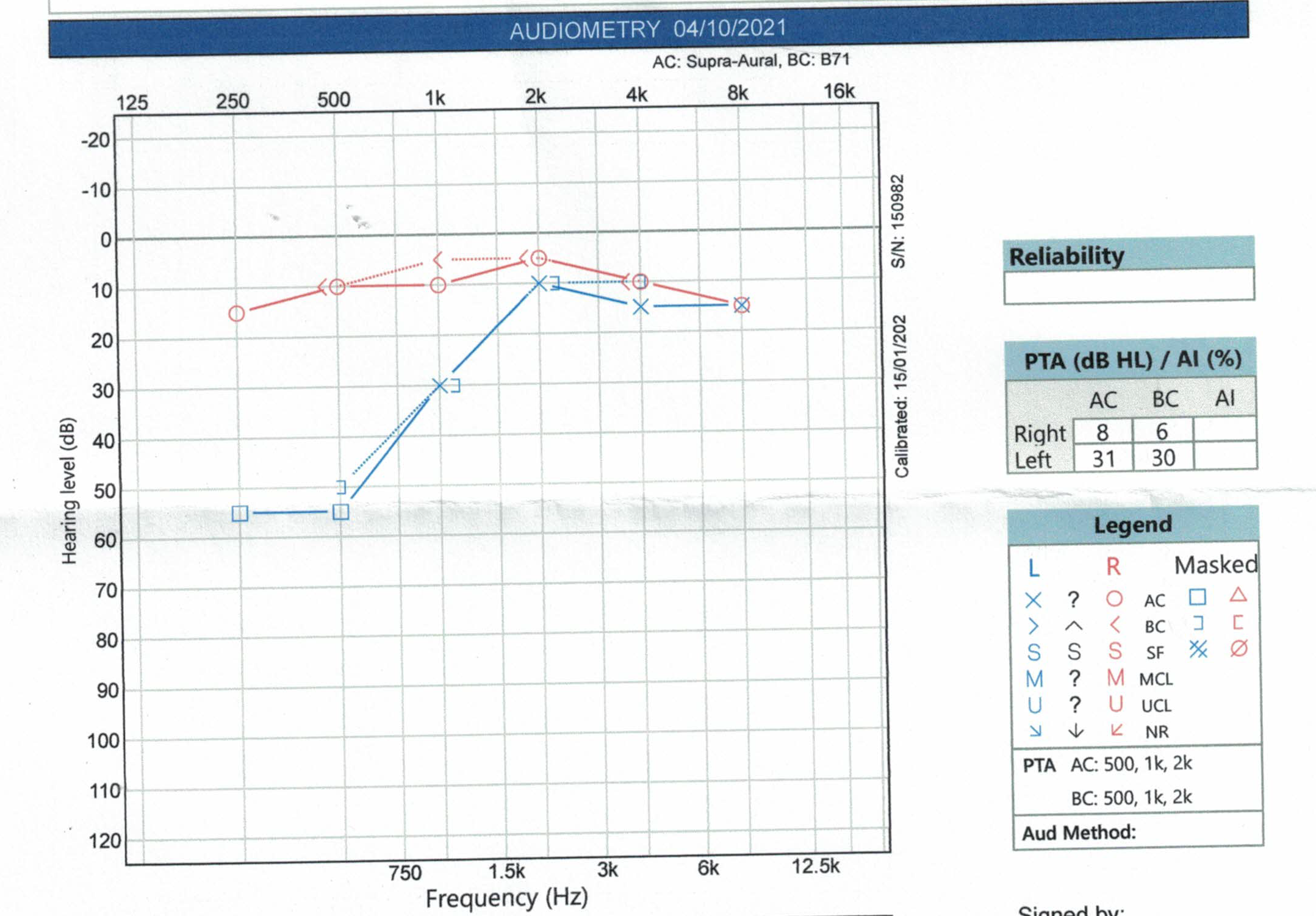
I commenced the patient on oral steroids with Betaserc and Valtrex. He made a very good recovery and this was his audiogram 19 days later.
Patients who have diabetes are not suitable for oral steroids and these patients should be offered steroid injections into the middle ear (intratympanic steroids, vidē īnfrā).
Hyperbaric Oxygen Treatment (HBOT)
Hyperbaric oxygen treatment is routinely used to treat divers who suffer decompression sickness. Over the past few decades, the field of hyperbaric medicine has found other conditions that respond well to this treatment. Sudden sensorineural hearing loss is one of these conditions. Hyperbaric oxygen treatment involves exposing a patient to 100% oxygen at pressures above sea-level atmospheric pressure (typically 1.5 to 2.8 atmospheres) in a specially designed chamber. The usual course of treatment is 10-20 one-hour sessions daily.
There is some evidence to support the use of hyperbaric oxygen in the first 2 weeks of the onset of sudden sensorineural hearing loss in combination with steroid treatment. For severe cases, this therapeutic window is extended to 4 weeks.
Intratympanic steroids
Intratympanic steroids involve the injection of a small volume of steroids (Dexamethasone or Methylprednisolone) through the eardrum into the middle ear under local anaesthesia. The procedure takes 30 minutes and the patient has to lie head down and refrain from swallowing following the injection. Intratympanic steroid injections are delivered 3-4 times over 1-2 weeks. The risks of the procedure include dizziness, discomfort, and rarely a persistent hole (perforation) of the eardrum.
The video below is a short clip of the procedure. As it is age-restricted, please click the “Watch on YouTube” link to see it.
At least 5 randomised control trials (RCTs) of intratympanic steroids in the salvage treatment of sudden sensorineural hearing loss (i.e. after initial treatment with oral steroids) suggest that improvement occurs in 37-48% of patients. One study which compared adding intratympanic steroids to oral steroids found no added benefit. So for now, intratympanic steroids should be reserved for patients who cannot take oral steroids (e.g. diabetics) or those who have not benefited from oral steroids. In this second group of patients, treatment with intratympanic steroids should begin within 6 weeks of the onset of hearing loss.
Case study 2
A 50-year-old man presented to me a month after the onset of left-side hearing loss. He had no other significant past medical history. He had seen another ENT soon after onset and was commenced on oral steroids and antivirals.
Following treatment, there was no improvement in hearing loss. He had an MRI scan and was advised to consider a hearing aid.
I commenced immediate treatment with intratympanic steroids. The first injection was 22 days after his first hearing test with the previous ENT. After 3 uneventful injections, his hearing returned to normal!
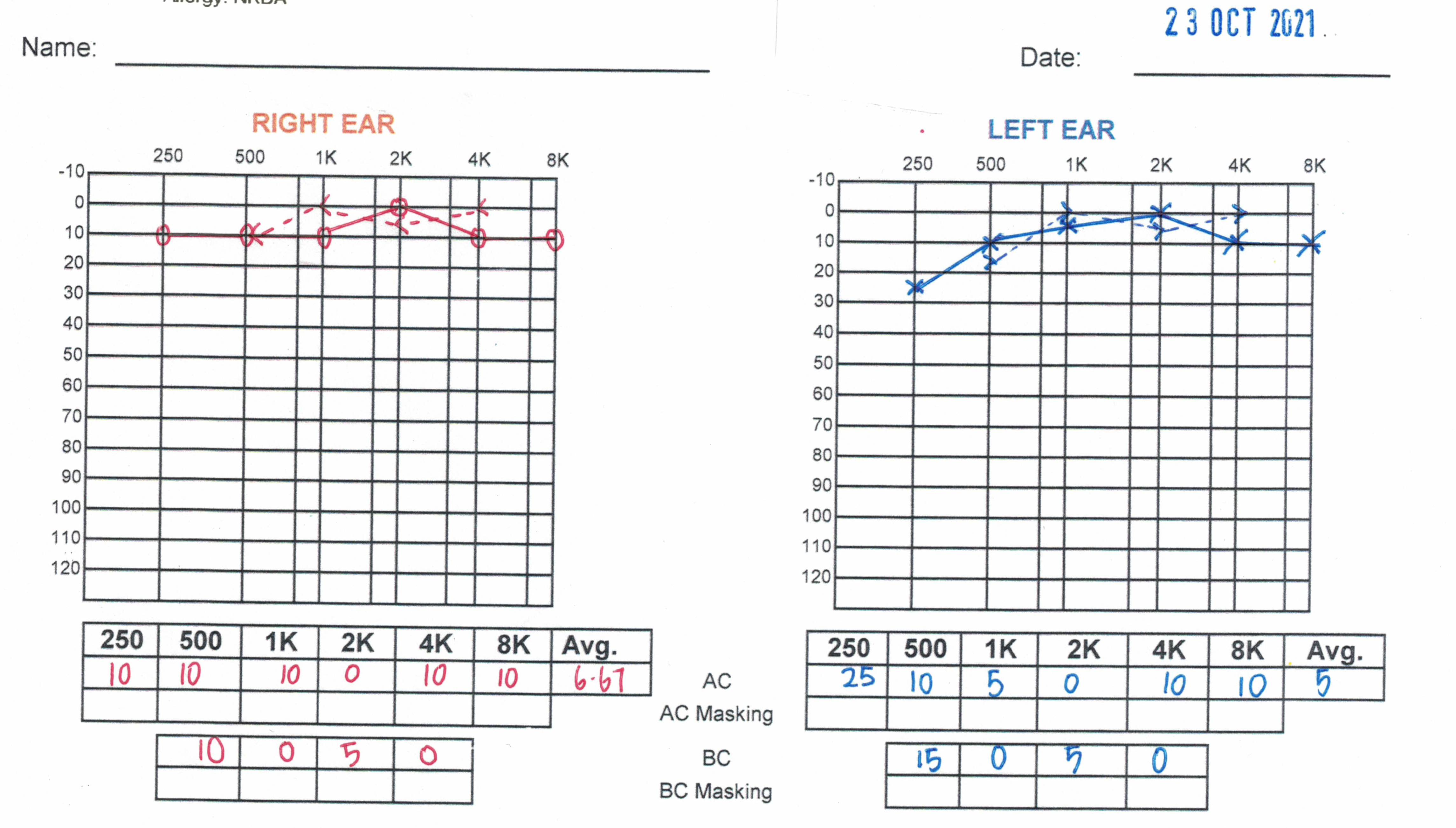
Whilst this case demonstrates the efficacy of intratympanic steroids, it is not the case with all patients. It is important though that your ENT specialist offers this option to you if oral steroids do not work. If he/she does not, see one that does!
Summary
- Sudden hearing loss which is often associated with ringing in the ear (tinnitus) is a real ENT emergency
- See a doctor as soon as possible and ensure that a cause is identified
- Find a doctor who can do a reliable tuning fork test or visit a hearing centre after a doctor has ensured that there is no wax in the ear canal or an infection causing hearing loss
- Consider oral steroids in all cases of sudden sensorineural hearing loss, but if you are diabetic ask about steroid injections into the middle ear
- Investigations such as an MRI scan and blood tests may be necessary but are not urgent as they do not influence initial treatment
[End]
Share this blog via:


