


Asymmetrical tonsils alone – not reason enough to remove them!
In the past few weeks, two children have been brought to see me by anxious parents worried about the apparent asymmetry in their children’s tonsils. In both cases the condition was spotted by the primary care doctors. The tonsils sit in the back of the throat. In most patients these tonsils are similar in size. Rarely, there is a significant difference in the size of the tonsils as depicted in the pictures below. In fact the prevalence of asymmetrical tonsils is about 1.7%.
Both these children were well but their parents and doctors were concerned about the risk of a cancer arising in the enlarged tonsil. Lymphomas are the most common head and neck cancer in children, and asymmetry of the tonsils is the most common manifestation of tonsillar lymphoma. Hence these concerns are not without reason.

Figure 1: This child’s right tonsil is larger than the left

Figure 2: View of the enlarged right tonsil via an endoscope passed through the nostrils. The leaf-like structure in the distance is the epiglottis which is part of the voice box
In 2015, a group in Brazil published a fairly comprehensive review of this subject and performed a meta-analysis of the published evidence. A meta-analysis looks at all the evidence, combines them and analyses them in a rigorous fashion. It provides by far the highest level of evidence to support a clinical recommendation.
One of the interesting observations is that many cases of asymmetrical tonsils diagnosed on simple inspection of the throat are not the case once they are removed! In several studies where ‘asymmetrical’ tonsils were removed, the tonsils were actually equivalent in volume in 39-52% of cases. In the remaining case, the tonsil perceived to be larger was more often than not smaller! The reason for this is not the skill of the observer but that several other factors determine how far towards the midline the tonsil protrudes. One of them is the depth of the tonsillar fossa or the bed in which the tonsil sits. And the second is the position of the anterior faucial pillar.
The meta-analysis helped generate likelihood ratios. The likelihood ratio (LR) of lymphoma was calculated for those patients with tonsillar asymmetry alone and those with tonsillar asymmetry and features of lymphomas such as discolouration or growth on the enlarged tonsil, swollen neck lymph nodes, recurrent fever, 10% weight loss, snoring, and swallowing difficulties. The LR of lymphoma in children with asymmetry alone was 43.5 but for those with asymmetry and symptoms it was 8938.4!
These likelihood ratios can be quite confusing to parents let alone clinicians! What they mean is that tonsil asymmetry alone should not be a reason to remove a child’s tonsils. But then what do we do with the asymptomatic yet asymmetrical tonsil?
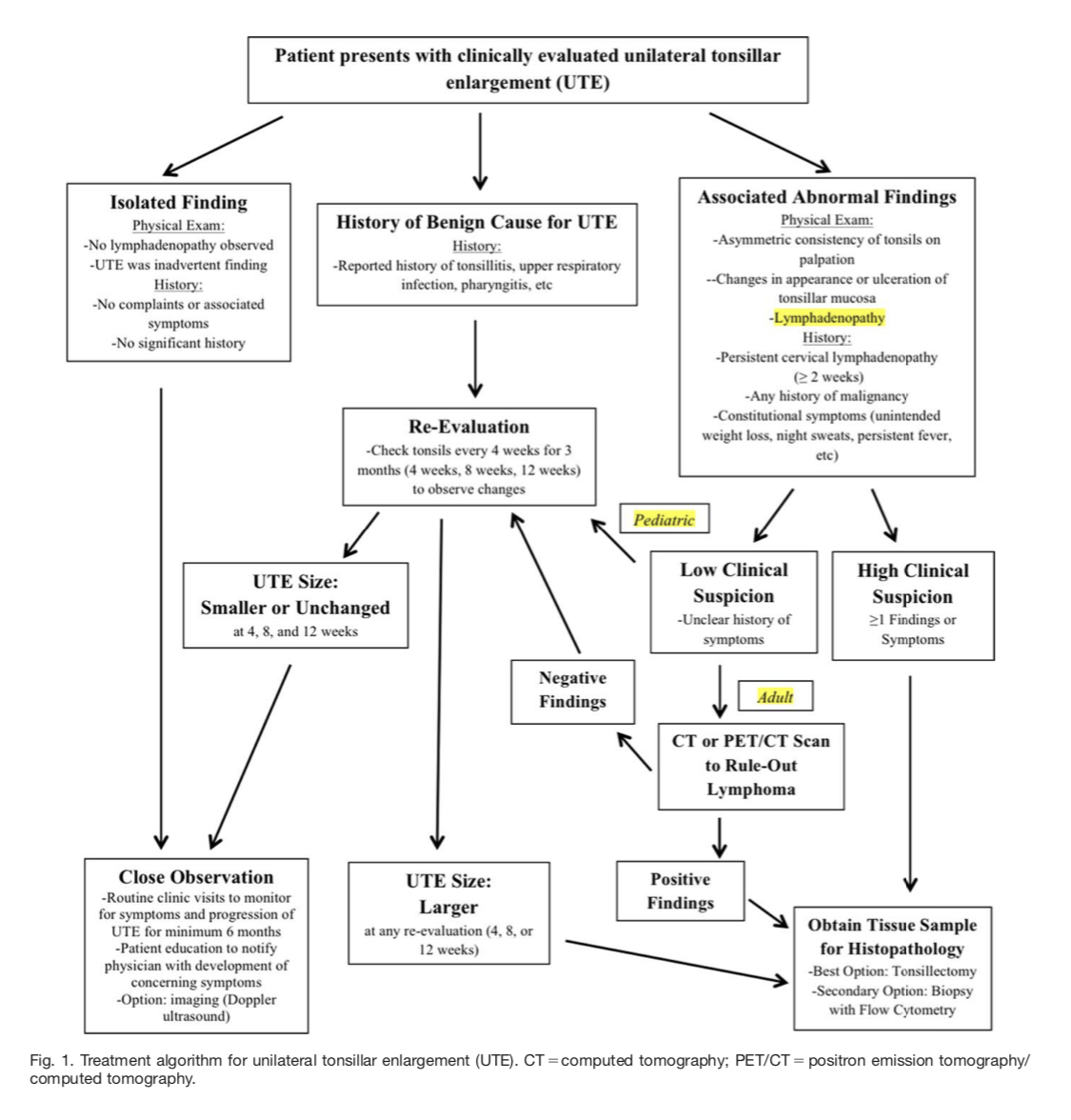
Michael Freidman’s group in Chicago published later in 2015 a very simple flow chart to help clinicians like me who faced two otherwise healthy young children who were now frightened by the anxieties of their parents. The flow chart below can be simply summarised to recommend a period of monthly surveillance for three months in patients with asymptomatic asymmetrical tonsils in whom there is a benign cause (e.g. tonsillitis) or absolutely no history suggesting an aetiology.
So – if you have managed reading this far – the knee jerk practice of removing all asymmetrical tonsils is without any basis. A surgeon who puts the fear of God into parents and children with tales of undiagnosed asymptomatic extranodal non-Hogkin’s Lymphoma is fear-mongering and best avoided!
JK
References
- Association between unilateral tonsillar enlargement and lymphoma in children: A systematic review and meta-analysis Alexandre Caixeta Guimarães; Guilherme Machado de Carvalho; Carlos Roberto Silveira Correa; Reinaldo Jordão Gusmãoa.
Critical Reviews in Oncology/Hematology 93 (2015) 304–311
-
What Is the Best Management of Asymptomatic Unilateral Tonsillar Enlargement? Michelle S. Hwang, BS; Kathryn E. Kaye, BS; Jonathan A. Waxman, MD, PhD; Michael Friedman, MD
Laryngoscope 125 (November 2015): 2438-2440
Share this blog via:


