


What to expect after my child’s adenoidectomy
Adenoids are a small pad of lymphoid tissue that sits right at the back of the nose. Lymphoid tissue is an integral part of the immune system. The adenoids, together with the tonsils, make up a ring of lymphatic tissue that encircles the back of the nose and mouth. This ring of lymphatic tissue is often called Waldeyer’s ring.
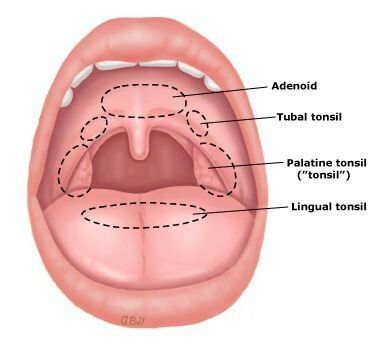
Waldeyer’s ring of lymphoid tissue which includes the tonsils and adenoids
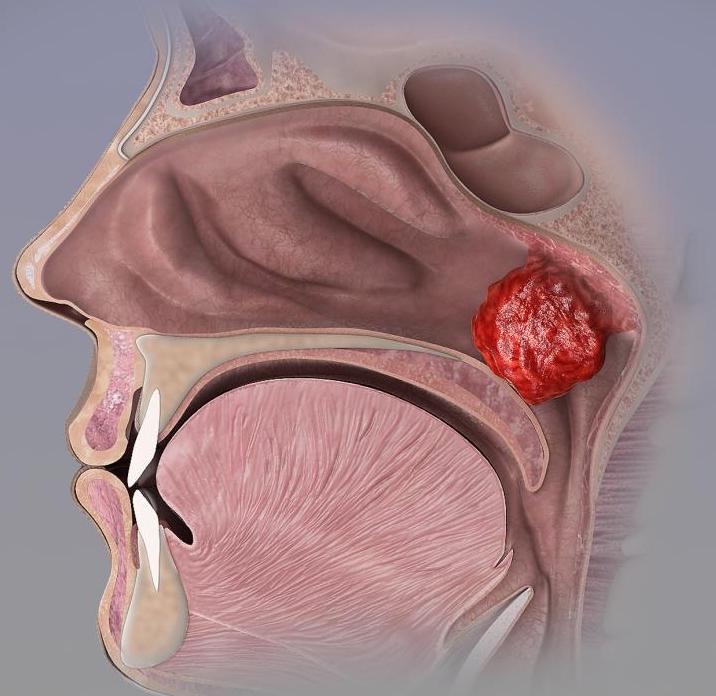
Enlarged adenoids in the back of the nose or in the nasopharynx. Image from Medical News Today
What purpose do adenoids serve?
Adenoids are important in the development of the immune system. Viruses and bacteria that are inhaled settle in the adenoids and stimulate the lymphatic tissue to produce antibodies and other immune cells that help fight infections. When one has an upper respiratory tract infection, the adenoids often appear inflamed. The image below shows chronically inflamed adenoids or adenoiditis. After the age of 3, adenoids are less important in the development and training of the immune system and therefore removal has few downsides.
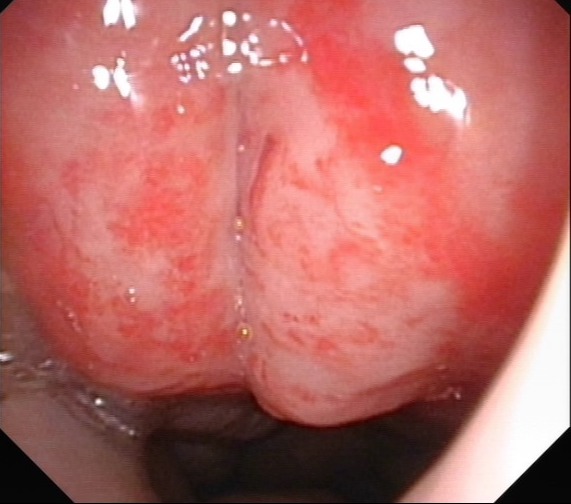
Inflamed and enlarged adenoids during a respiratory tract infection
What problems can adenoids cause?
Adenoids are naturally large between 3-8 years of life. In some children, the adenoids are excessively and persistently enlarged and start to pose problems. Enlarged (or hypertrophic) adenoids cause nasal obstruction and mouth breathing. This affects a child’s quality of sleep. Sleep is restless with frequent arousals. Mouth breathing also affects the growth of a child’s face and jaw. The face is said to be ‘long’, the mouth perpetually in the open position, and the lower jaw recessed. This is often described as the adenoid facies.
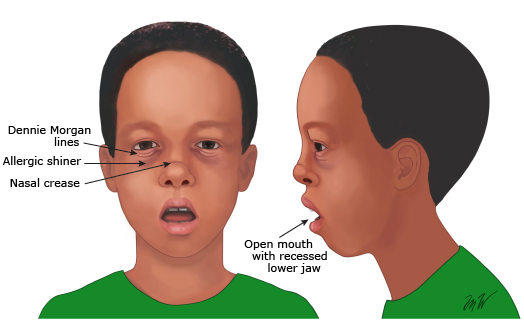
The long face associated with mouth breathing and nasal obstruction. Nasal blockage can be due to allergies and hence associated with Dennie-Morgan lines, allergic shiners, or a nasal crease. Image from UpToDate
Large adenoids can also block the opening of the eustachian tube that connects the back of the nose to the middle ear. This predisposes to recurrent ear infections or an accumulation of thick fluid in the middle ear which causes hearing loss. The build-up of thick fluid in the middle ear is often called glue ear or otitis media with effusion (OME). This condition is painless but hearing loss can lead to speech delay.

Thick fluid behind the left eardrum in this 4-year child caused hearing loss and speech delay
How do I know if my child has large adenoids?
Assessment of adenoids is best undertaken by nasal endoscopy. This is a simple investigation where a child’s nose is anaesthetised with a nasal spray and the surgeon inserts a flexible fibreoptic scope into the child’s nose. Some children find this investigation difficult. They do have to remain still and keep breathing to the nose during the examination. Breathing through the mouth or crying raises the soft palate and overestimates the size of the adenoids. An alternative to nasal endoscopy is an x-ray.
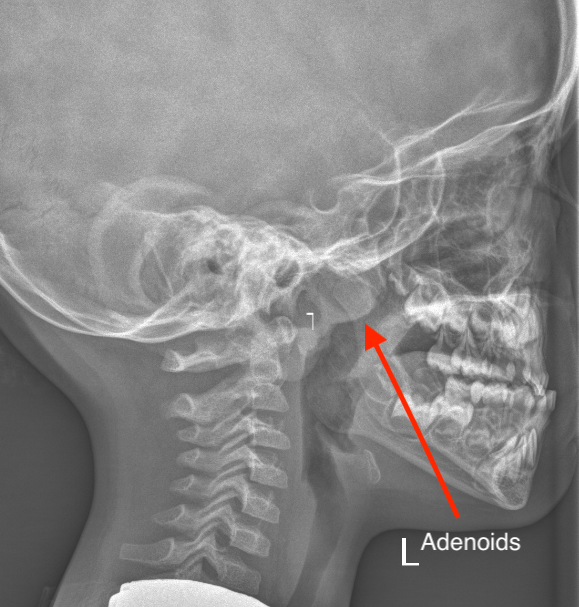
A simple x-ray. The adenoids are mildly enlarged (red arrow)
Can enlarged adenoids be treated without surgery?
I often try and treat enlarged adenoids by non-surgical means. Mild enlargement may not require any treatment at all. Addressing allergies is important as adenoid enlargement is driven by allergies. There is evidence to support the use of nasal steroid sprays in shrinking the adenoids. In fact, one study showed that 3 of 4 children advised to have adenoidectomy eventually responded to these sprays and did not need surgery (see ref 1). It is worth trying nasal steroids in some cases. The common sprays are Nasonex and Avamys.
Another drug that has been proven to help with adenoid enlargement in Montelukast or Singulair. This is an antileukotriene and it has been shown to reduce adenotonsillar inflammation and obstructive sleep apnoea (see ref 2). Montelukast is associated with some side effects suggest as mood change. I am therefore a little cautious when advising the use of this drug on a long term basis.
Adenoidectomy
Adenoidectomy is a common operation in children. It is performed under general anaesthesia and may take 30-45 minutes. In 2017, the American Academy of Otolaryngology/Head and Neck surgery stated the following indications for adenoidectomy:
- Four or more episodes of yellow or green nasal discharge in a child under 12 over the preceding 12 months
- Persisting symptoms of adenoiditis after two courses of antibiotics
- Sleep disturbance with nasal blockage persisting for at least 3 months
- Hyponasal speech
- Glue Ear for over 3 months especially in children over 4 years
- Dental malocclusion or facial growth disturbance documented by orthodontist or dentist
Parents of children undergoing adenoidectomy may come into the operating theatre with their child. Once general anaesthesia is induced the parents are escorted to a waiting area. The child will have a breathing tube inserted into their windpipe (endotracheal intubation) for the procedure.
I usually undertake adenoidectomy using coblation or controlled ablation. This is guided by endoscopy, so a scope is placed in through the nose, and the coblator ‘wand’ is passed into the mouth and behind the soft palate to reach the adenoids. The wand sucks and ablates the adenoids. The temperature of the probe tip is only 70 degrees so thermal damage is minimal.
This is a video of an adenoidectomy. You may want to skip this if the sight of blood (albeit small amounts) makes you queasy
After the operation, you will be able to join your child in the recovery room. Your child will be placed in the recovery position (i.e. lying on his/her side). The operation is not a painful operation (assuming it is not done with a tonsillectomy). They may however be a little upset as they awake from anaesthesia.
Post-operative care
Once your child is fully awake, they will be returned to the ward for further monitoring. The main thing to look out for is for any bleeding. Some blood or blood-stained nasal mucus or saliva is to be expected. The nose may appear to be very congested. In fact, it may appear to be blocked. Do not worry about this as will settle over the course of the first week.
Complications
- The main risk of adenoidectomy is bleeding following surgery. Large studies have shown this rate to be 0.5-0.8%
- Some children will have an altered voice (hypernasal speech). This is often transient and resolves
- Neck pain with rotation or neck spasm is a rare complication
What to expect following discharge
If your child has only had an adenoidectomy, it is likely that you will be discharged on the same day of surgery. Pain is often minimal. Nasal congestion may still persist and you may be advised to use nasal salt water sprays or decongestants. If your child has co-existent allergies then antihistamines may be prescribed. Most patients will also receive antibiotics. Most children do not need more than 3-5 days away from school. They can start swimming after 1 week. Most activities can be resumed in 5 days.
Can adenoids regrow?
One of the concerns with adenoids – which is not the case with tonsils – is the risk of regrowth. The rate of adenoid regrowth with modern techniques of adenoidectomy is 1.5%. In children under 5, the rate of regrowth is 2.5 times greater. So some children, albeit a minority, may need their adenoids removed again.
I hope this information is helpful. Whilst a lot of information here is from learned medical journals and textbooks, the really useful stuff is what I learn from parents! So if you feel I have missed something out and wish this communicated to other parents, please do email me at drjeeve@entclinic.sg
References
- Demirhan H, Aksoy F, Ozturan O, Yildirim YS, Veyseller B. Medical treatment of adenoid hypertrophy with “fluticasone propionate nasal drops”. Int J Pediatr Otorhinolaryngol. 2010;74(7): 773–6.
- Kar M, Altintoprak N, Muluk NB, Ulusoy S, Bafaqeeh SA, Cingi C. Antileukotrienes in adenotonsillar hypertrophy: a review of the literature. Eur Arch Otorhinolaryngol. 2016;273(12):4111–7.
END
Share this blog via:


