


The child with a blocked left nostril
Earlier this year, I saw a 13 year old child with an unusual complaint. He presented with nasal blockage that was entirely left sided and told me that his nose “was only blocked when he breathed out”. Truly enough in clinic he demonstrated to me that he could breathe in through his left nostril without difficult but could not breathe out. He had been seen by his family GP who duly prescribed a nasal steroid spray. This had no effect on his symptoms, so he was referred on to me.
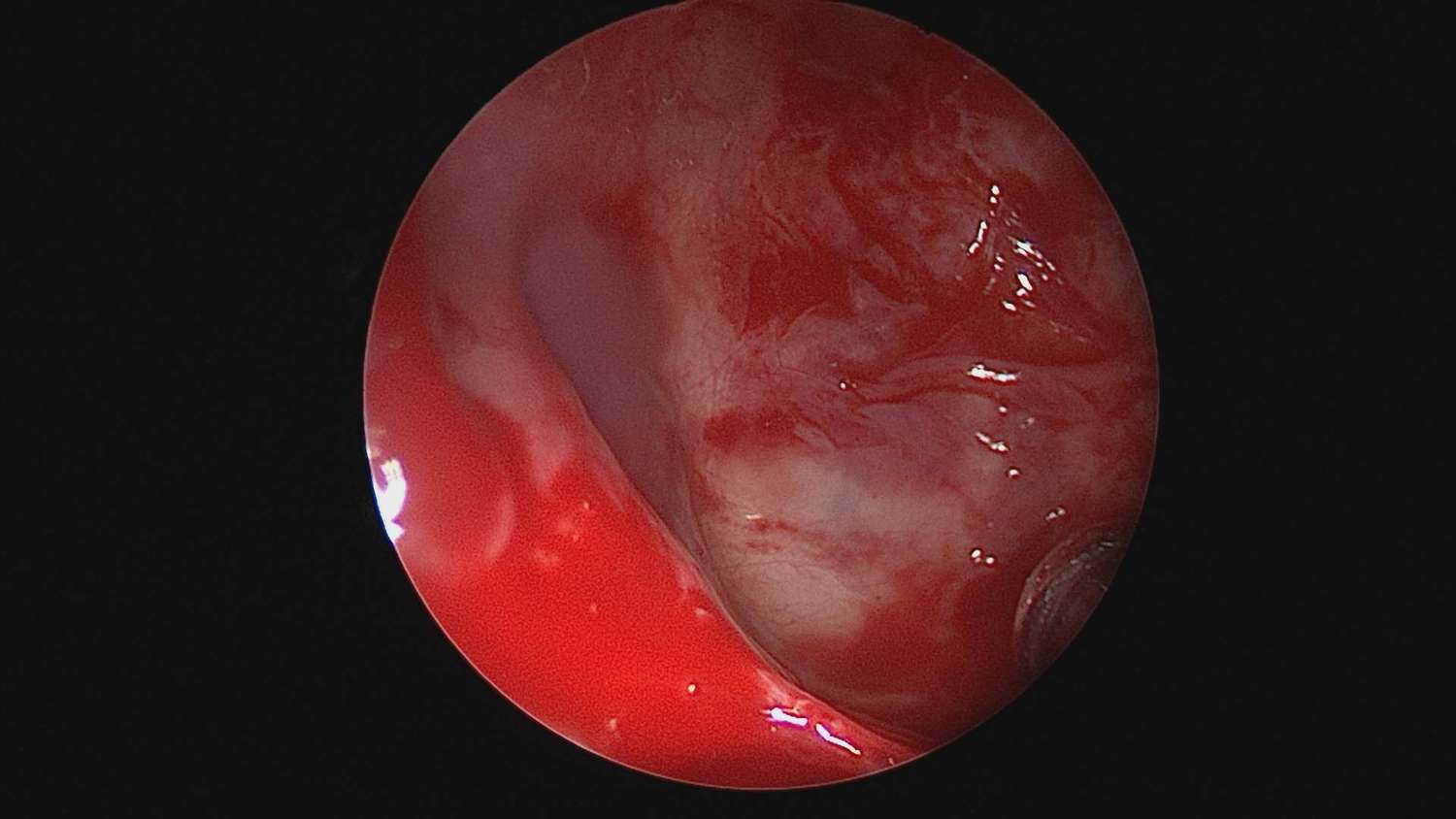
I examined him with a nasal endoscope and this was what I found in his left nasal cavity

Left nasal cavity. The wall between the nasal cavities or septum in on the left, and in the distance you can see a pale fleshy polyp

Closer view of the polyp
What I saw was in fact just the ‘tip of the iceberg’. As this subsequent CT scan showed, the polyp arose in the left cheek or maxillary sinus. These polyps are called antrochoanal polyps as they arise in the maxillary antrum and expand into the nasal cavity towards its back end or choanae.
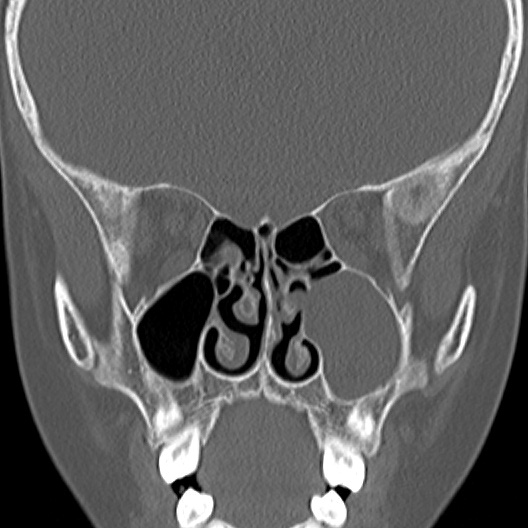
CT scan of the child showing that the polyp arose in the left cheek sinus and what I saw in the nose was merely the ‘tip of the iceberg’!
Antrochoanal polyps are different from nasal polyps. They are almost always one sided and often occur in younger adults and children. These polyps are sometimes called Killian polyps. The portion that is in the cheek sinus (maxillary sinus) is invariably cystic and the portion visible in the nose is solid. These polyps cause a classic ‘ball-valve’ obstruction of the nasal passage, hence the ability to breathe in, but not out. There is no obvious cause for these polyps. As a rule, one sided polyps in children merit some form of imaging to exclude a rare condition called a meningo-encephacoele. Meningo-encephalocoeles are due to a defect in the base of the skull resulting in herniation of brain and its lining into the nasal cavity. So all one sided nasal polyps in children should be treated with caution, and a meningo-encephaocoele should be excluded by imaging the sinus and skull base. My chosen modality of imaging is actually an MRI scan which does not expose the child to radiation. In this case we attempted an MRI but due to claustraphobia, we obtained a simple CT scan instead.
Surgery is the gold standard of treatment and simple avulsion in clinic of the nasal portion is often insufficient. Endoscopic removal through the nose is best and often it is necessary – as was the case in this child – to fashion an adequate opening or antrostomy.
The opening into the cheek (maxillary) sinus following removal of the polyp
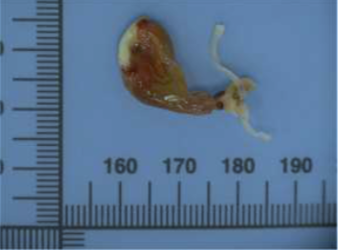
The polyp following removal. Notice the solid portion and the lining of the cystic portion that lies within the cheek (maxillary) sinus
The operation went smoothly in this child and he made an excellent recovery. I recently saw him for a review. He was breathing much better and sleeping peacefully! When I examined the nose, the polyp had not recurred and the opening to the maxillary sinus was widely patent.
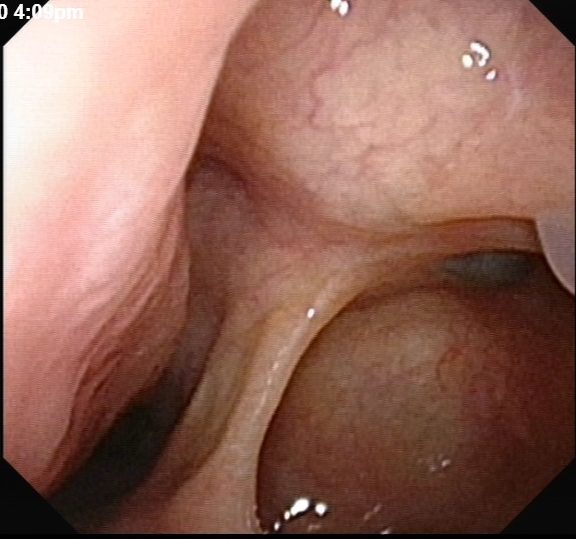
The healed post-operative view of the left nasal cavity and opening into the maxillary sinus
Share this blog via:


