


Hearing loss and “Glue Ear” in Children
Hearing loss is common in children and may often go unnoticed. Just a few days ago a parent brought a child to see me for a sore throat. The child, she said also had a wax problem for which her family physician had attempted syringing. Her mother said that there was no hearing loss. I enquired about speech development which had been normal. But on further probing her mum said that she did have some inattention at times. This was thought to be duet to “selective hearing”
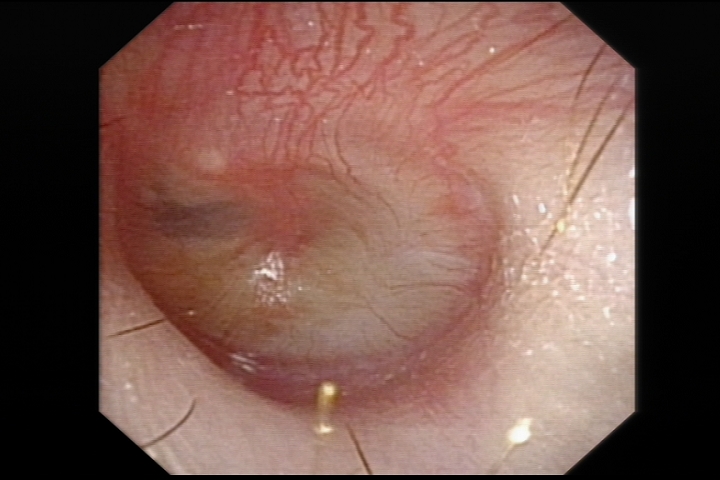
On examination, her eardrum appeared opaque and on closer inspection there was fluid in the middle ear with an air bubble clearly visible
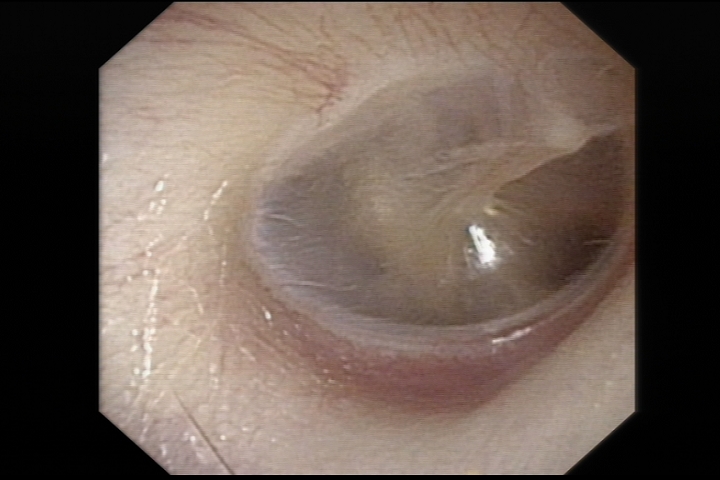
Compare this to a health eardrum in another child
This fluid in the middle ear – behind the eardrum – causes a small ‘conductive’ hearing loss. It is not unlike listening to people with your ears submerged in water. Some children may tug at their ears because of this. If long standing, there may be some speech delay. This is especially so in children under 3 who are starting to learn to speak.
Middle ear fluid may be present after a simple ear infection and it may takes several weeks to resolve. If it persists for 12 weeks or more it is considered chronic and the term “glue ear” is applied. In these children, the tube that connects the middle ear to the back of the nose – the “Eustachian tube” – functions poorly.
There are many strategies to overcome this problem. Treating nasal allergies does help improve the Eustachian tube’s function and may help middle ear fluid resolve. Another device which helps is something called the Otovent. There are several ways to use this device, the youtube links below show how to use the Otovent device. The second video by Dr Douglas Mann of Cape Cod, Massachusetts gives a detailed description on how the device works.
https://www.youtube.com/watch?v=oi6DdairDIo
In cases where this conservative measure fails, a grommet insertion may be necessary. Grommets or Ventilation Tubes are small teflon tubes that are inserted through a small cut made in the eardrum (a myringotomy). It allows for middle ear fluid to be suctioned dry and then allows the middle ear pressure to equalise with environmental pressure.
The UK TARGET trial (Trial of Alternative Regimes in Glue Ear Treatment) reported in the 1990s that insertion of Ventilation Tubes should be done in children with persistent fluid in the middle ear after 12 weeks of watchful waiting. In cases where there is speech delay, it may be wise to expedite tube insertion.
Grommets insertion is a short procedure which can be done as a day case. It requires a general anaesthetic. It is fairly safe. The British ENT Society suggest abstaining for swimming for 2 weeks after grommet insertion. Care must be taken with dirty or soapy water entering the ears. Whilst the tubes are in, there is a risk of infection and chronic discharge of pus from the ears. The tubes fall out after 9-12 months. In most cases the hole in the eardrum then closes spontaneously. Very rarely, a persistent hole may remain.
About 5% of patients will need a second set of grommets. When this is done, It is wise to have the child’s adenoids removed at the same time to improve Eustachian tube function.
Share this blog via:



