


Thyroid nodules – when to be concerned…
The thyroid gland is situated in the front of the neck like a shield of a warrior protecting the windpipe or trachea which lies behind it. Indeed the word thyroid is derived from the Greek word for shield. The butterfly-shaped gland produces a hormone called thyroxine which is involved in the regulation of a variety of bodily functions. In essence, it controls your ‘metabolic rate’, so patients with low levels of thyroxine feel tired, lethargic and gain weight. Whilst those with high levels – a condition called thyrotoxicosis – suffer from sleeplessness, weight loss, palpitations and tremors.
The thyroid gland is prone to developing small lumps within it which are called nodules. These may appear gradually or suddenly. Occasionally they may be painful. Figure 1 shows a gland with several large nodules – a common condition known as multinodular goitre. About 60% of women will have a thyroid nodule present if they were to have an ultrasound scan of the neck. The vast majority of these nodules are benign but may require treatment if they cause swallowing or breathing problems. However, 5-10% of nodules may harbour a cancer and therefore require surgical removal. Trying to decide which nodules are sinister is challenging.

Figure 1: A large multinodular thyroid gland
To decide if a nodule has a cancer within it, surgeons frequently use ultrasound scans and then take a small sample of cells from the nodule with a needle. Ultrasound can identify worrying features which signify cancerous change. There are now newer advanced applications such as elastography which help identify malignant nodules (see Figure 2). The cells sampled from a needle biopsy are analysed by cytologist to help make a diagnosis (see Figure 3). More recently, special molecular diagnostic techniques which identify point mutations in genes can help in the identification of malignancy. These include mutations in the BRAF and RAS genes.
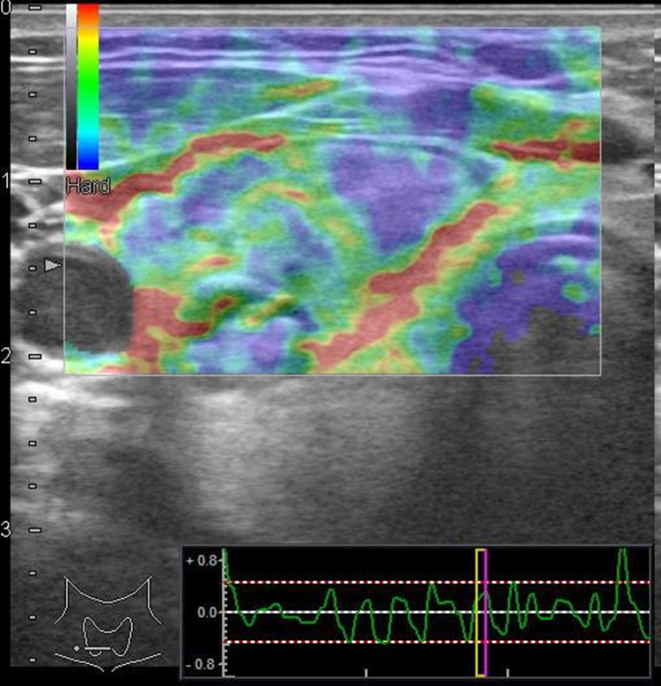
Figure 2: Ultrasound using elastography promises to identify malignant nodules based on their compressibility
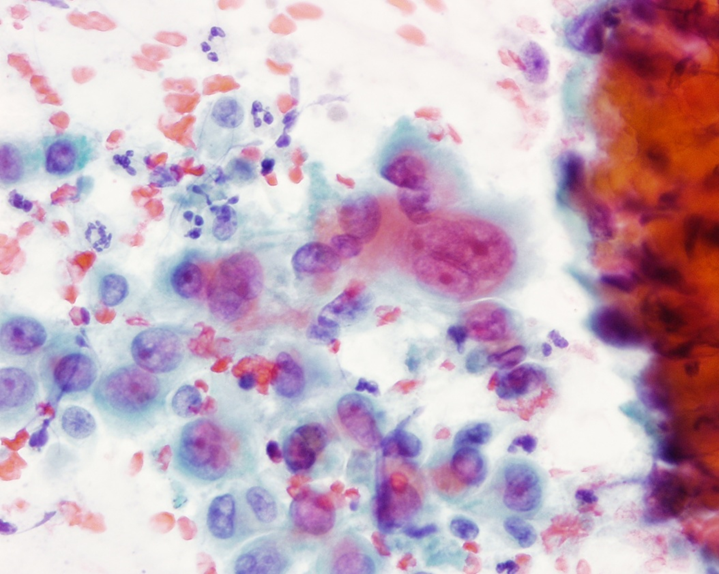
Figure 3: A cytology smear to help make a diagnosis
Once a nodule is deemed to be of concern, surgery is often advised. Surgical removal of the thyroid gland is known as thyroidectomy. If the nodule is clearly cancerous, the entire gland is removed in an operation called total thyroidectomy. This is a common operation, first performed by Professor Theodor Billroth in the 1860s in Europe. If the nodule has worrisome features based on the ultrasound scan or biopsy, some surgeons may choose to remove just half the gland first in an operation known as hemithyroidectomy or thyroid lobectomy. The nodule may then be sent for further analysis before the surgeon proceeds with further surgery.
The technique of thyroidectomy has evolved substantially. Technology has made this surgery safer and more effective. Amongst the more notable improvements is the use of nerve integrity monitoring which reduces the risk of nerve damage during which may affects the patient’s voice. The harmonic scalpel is another instrument which reduces blood loss from surgery and is associated with less pain following surgery.
The scar following thyroid surgery often heals well. Whilst it may appear unsightly initially, most people heal well and the scar is often imperceptible several months after surgery.
Share this blog via:



